“I want whatever works best."
"I'll take whatever they have at the pharmacy."
"Is there a difference?"
I bet you’ve heard similar responses when talking to your patients about emergency contraception (EC). How can we to address these responses? How do we help our patients make the best decision they can for their emergency contraception?
What works best?
First off, the most effective EC for anyone is the copper intrauterine device (IUD). A systematic review of 35 years of data from using the copper IUD as EC showed a failure rate of less than one per 1,000. The copper IUD also has no loss of efficacy with an increase in body mass index (BMI), so it is a particularly good choice for obese women presenting after unprotected sex. It also remains highly effective when inserted up to 5 days after unprotected intercourse (UPI ), unlike EC pills. Finally, the copper IUD has the added benefit of providing long-term contraception.
What do we know about weight and EC pills?
The concern about the efficacy of hormonal EC and weight stems from a meta-analysis of two randomized controlled trials comparing the efficacy of two kinds of EC pills: levonorgestrel (LNG, like Plan B One-step, Next Choice, and other generics) versus ulipristal acetate (UPA, like ella).
Among LNG pill users, the study found that the risk of pregnancy was more than four-fold greater for obese women compared with women with normal BMI. In fact, levonorgestrel showed such a rapid decrease of efficacy with increasing BMI that for women with BMI at 26 or higher there was no effect on pregnancy prevention.
Among UPA pill users, the risk of pregnancy was two and a half-fold greater for obese women compared to women with normal BMI. For UPA, there was no effect on pregnancy prevention at BMI of 35 or greater.
This study also conducted analyses using weight rather than BMI, and those analyses came to a similar conclusion—higher weight meant less effective EC pills.
These data led the makers of an LNG pill in Europe known as NorLevo to change their label. It now warns: “In clinical trials, contraceptive efficacy was reduced in women weighing 75 kg (165 lbs) or more, and levonorgestrel was not effective in women who weighed more than 80 kg (176 lbs).” Thus far, neither the manufacturers nor the United States Food and Drug Administration (FDA) have made changes to the labels for EC pills sold in the U.S. However, more research on this topic is forthcoming and if the new studies confirm these findings, label changes may be just a matter of time.
What does this mean for your patients?
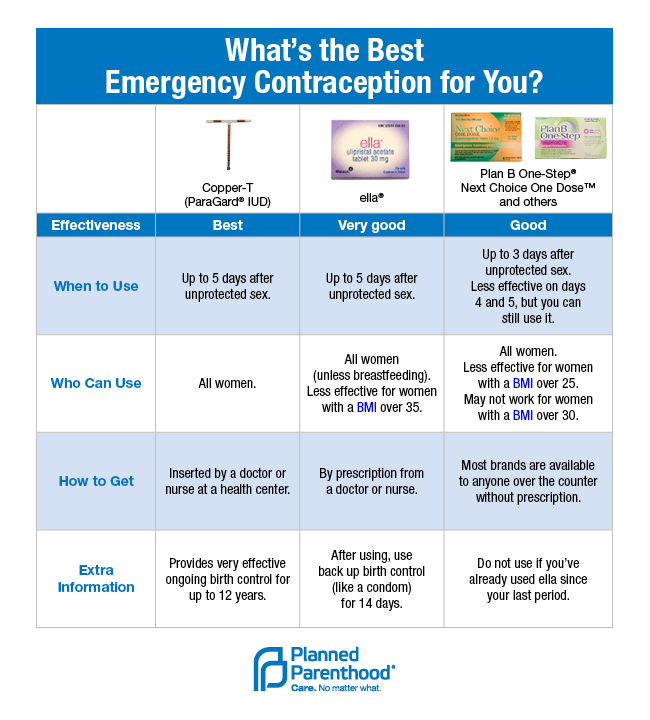
Given these new data on the relative efficacy of different types of EC, clinicians should consider starting EC counseling with the copper IUD. If you’re already using tiers of effectiveness for contraceptive counseling, you can apply the same approach to EC. Here are patient education charts showing EC options in order of their effectiveness.
If your practice is not already offering IUD insertion at a patient’s first visit, you may have some challenges to offering the copper IUD for EC. For example, you need to have the devices in stock, have providers on staff who are comfortable with the insertion procedure, and have time in your schedule for the slightly longer appointment. Clinics around the U.S. have committed to offering the copper IUD for EC as part of a special project of the National Family Planning & Reproductive Health Association. These clinics are working through these types of challenges, and they’ll be sharing what they learn in the coming months.
For women who can’t use the copper IUD or choose not to, you can help them choose between LNG and UPA based on their BMI, time since UPI, and access. Women with BMI >=26 or more than 3 days elapsed since UPI should be counseled to take UPA since it does not decrease in efficacy for up to 5 days. LNG should be reserved for women with normal BMIs who are able to take EC soon after UPI, and for those for whom access to UPA is not feasible. Overall, these new data about EC are good news. They allow us to give our patients more accurate information about their options and encourage us as providers to expand our services to meet our patients’ needs. Stay tuned for more information on EC effectiveness in the coming months!
Grace Shih, MD, MAS is a family practice physician in Seattle, WA. She completed her family medicine residency at Brown University and her family planning fellowship at University of California, San Francisco. When she's not seeing patients, you can find her cooking, hiking, or salsa dancing.



{kind=link}