




The scenario:
A patient in your clinic is requesting to have an LNG-IUD placed today. You note that their last menstrual period (LMP) started 10 days ago, and when asked about recent unprotected vaginal intercourse, they report they last had sex three days ago.
What do you need to consider before placing an IUD today?
Questions about when to start birth control, including when to offer emergency contraception (EC), come up in practice every day and improving same-day access to a patient’s birth control method of choice relies on getting the right answers. When placing an IUD, providers should consider a patient’s history including LMP, risk of pregnancy at last sexual encounter, and need for EC. If none of the six CDC criteria on “how to be reasonably certain that a client is not pregnant” are met, consider checking an in-office urine pregnancy test, as research supports offering people with a negative pregnancy test the option to have their IUD placed now because of the low risk of pregnancy.
When can I place an IUD after unprotected vaginal intercourse?
There are currently four LNG-IUDs (Mirena, Liletta, Skyla, and Kyleena) and one copper IUD (Paragard) on the market in the US. Research supports the use of LNG-IUDs with 52mg of levonorgestrel (Liletta or Mirena) as highly effective EC—more than 99% effective in preventing pregnancy when placed anytime within five days of unprotected sex. That means that both the copper IUD and LNG 52mg IUDs can now be used as EC. The other LNG-IUDs (Skyla and Kyleena) have not been tested for EC.
A growing body of research shows that people have a low risk of pregnancy (<1%) when starting a copper or LNG 52mg IUD after unprotected vaginal intercourse anytime in the menstrual cycle with a negative urine pregnancy test. This is important because >40% of IUD EC users have had unprotected sex multiple times in the last two weeks and commonly more than five days prior to IUD placement. For decisions about placing a copper IUD or a LNG 52mg IUD after unprotected sex at any time in the menstrual cycle, check an in-office pregnancy test and engage patients in shared-decision making conversations—weighing the less than 1% risk of pregnancy in the month of placement with the risk of future unintended pregnancy if they leave without an IUD and are told to come back later.
Can the patient in this scenario get their IUD today?
Yes. This newly published research means that the patient in this scenario can have their IUD placed today without the need for another method of EC, such as Plan B or generic LNG-EC pills, and continue using it as birth control without the need for a back-up method.
What is the “best” EC method?
EC should be offered to anyone who is capable of becoming pregnant, has had unprotected or under-protected vaginal intercourse in the last five days, and does not desire pregnancy. There is no one best method of EC for all patients or in all scenarios. Decisions about selecting an EC method depend on patient preference, availability of EC methods, patient factors such as body weight, provider training to offer all methods of EC, and the potential interaction of ulipristal acetate (ella) EC pills and progestogen-containing contraception (aside from the LNG IUD).
While a copper IUD or LNG 52mg IUD are the most effective EC methods regardless of body weight and the only EC methods that continue to work as ongoing contraception, they require a visit with a health care provider who is trained to place them, take the most time to obtain, and are the most expensive for those without insurance coverage. In addition, some people simply do not want an IUD.
For a patient who is a candidate for EC but does not want an IUD, either at all or for EC, you can offer over-the-counter levonorgestrel EC pills, such as Plan B or generics, or a prescription for ulipristal acetate (ella) as EC (which is more effective but requires a prescription).
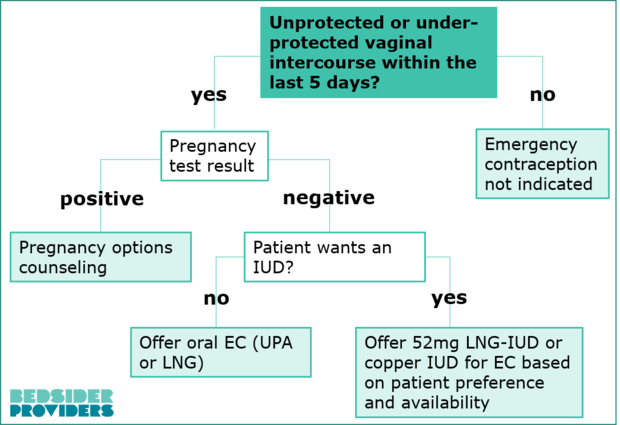
Use this quick chart to help you make decisions about offering IUDs as EC in your practice:
What counseling is needed for patients who use an IUD for EC?
When using an IUD as EC, provide patients with all the standard counseling on changes in bleeding patterns, maximum duration of use, lack of STI protection, and presence of strings. It is important to let patients know that they can have their IUD removed at any time. Additional counseling points when using an IUD as EC include:
- It’s effective right away—no back-up method needed. When using an IUD for EC there is no need to use a back-up method of birth control, such as condoms, to prevent pregnancy.
- An LNG 52mg IUD can affect bleeding patterns. Using an LNG-IUD, as EC or ongoing birth control, can change bleeding patterns, including increased bleeding and spotting in the first few months after placement. (This is usually followed by a decrease or no bleeding for the rest of use.)
- A copper IUD won’t change when a patient gets their next period but can cause bleeding or spotting before then. While EC pills and an LNG-IUD can change the timing of a patient’s next period, placing a copper IUD doesn’t significantly change the timing of their next period when used as EC (or as birth control).
- Patients should take a pregnancy test two to four weeks after using an IUD as EC. Patients should take a urine pregnancy test two to four weeks after IUD placement (or anytime they have signs of pregnancy), either at home or in the office.
What follow up is needed after using an IUD for EC?
All EC methods work by preventing pregnancy and are not the same as an abortion. And no method of EC changes the chances of getting pregnant in the future (once an IUD is removed). However, pregnancy is possible after using EC pills or an IUD. Patients with an IUD who have a positive urine pregnancy test should be advised to contact their provider for IUD removal and should be offered pregnancy options counseling, including connection to requested care for abortion or prenatal care.
Key Points
- EC, including IUDs and EC pills, are safe for most patients and are an important option for pregnancy prevention after sex has occurred.
- Providers can place either a copper IUD or an LNG 52mg IUD up to five days after unprotected or under-protected vaginal intercourse as an effective method of EC.
- A growing body of data supports IUD placement at any time during the menstrual cycle with a negative urine pregnancy test, regardless of the timing of unprotected sex.
- Engage patients in shared-decision making conversations about the timing of IUD placement to weigh the risk and benefits of placement today.
- Patients can continue using a copper IUD or LNG 52mg IUD as ongoing contraception—no backup method needed.