




The shot, a.k.a. depot medroxyprogesterone acetate (DMPA), brand name Depo-Provera or “depo” for short, is a highly effective, progestin-only injectable birth control method that prevents pregnancy for three months after it’s given. The shot comes in two equally effective formulations, one is given intramuscularly (IM) and the other subcutaneously (SQ). Both types can be given in a clinic or health care setting, but DMPA-SQ was originally designed for administration at home by the user or a trusted contact. Self-injection offers greater autonomy and reduces barriers to care by eliminating the need to return to a health care setting every three months for re-injection. Additionally, DMPA-SQ is given with a smaller needle and less volume of medicine than the IM injection, decreasing pain for some users.
While several studies in the US and globally have demonstrated safety and feasibility of DMPA-SQ given outside of a health care setting, DMPA-SQ is labeled by the Food and Drug Administration (FDA) “only to be administered by a health care professional.” (Update May 2021 — the CDC now recommends self-injection of DMPA-SQ!)
Who can use DMPA-SQ?
Anyone who can use the shot for birth control can use DMPA-SQ, regardless of age or if they have ever used the shot for birth control before. Good candidates for self-injection include people who are experienced in self-injection of other medications such as those used to induce ovulation for IVF, multiple sclerosis, or insulin for diabetes, but experience with self-injection is not a prerequisite for using DMPA-SQ.
Prescribing DMPA-SQ
You can prescribe DMPA-SQ after a telehealth or in-person visit, depending on your patient’s preference and availability. DMPA-SQ can be started at any time you can be reasonably certain that someone is not pregnant. This Quick Start Algorithm supports providers’ decision making about starting or restarting birth control at any time during the menstrual cycle, including considerations for emergency contraception.
Send a prescription to the client’s pharmacy of choice for a one-year supply of depo-subQ Provera 104 (104 mg/0.65 mL) (NDC code 0009-4709-13) for 4 refills q 3 months. In some states, you may have to prescribe a sharps container and alcohol pads but in others, people can request these items directly from their pharmacy. The effectiveness of DMPA-SQ is not impacted by body weight, so there is no dose adjustment needed.
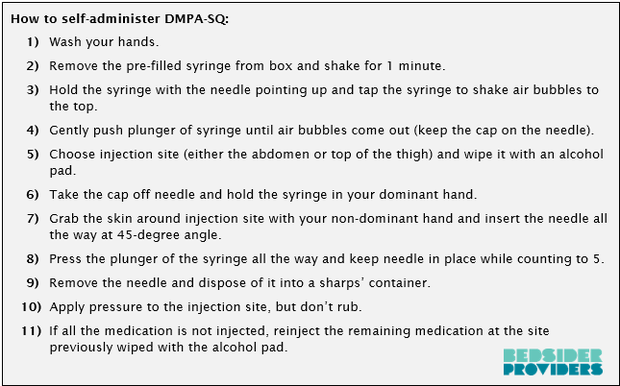
Administering DMPA-SQ
Patient education and counseling about how to administer DMPA-SQ can be done via telehealth or in person, depending on how the user learns best and appointment availability. You can even send educational videos and written material for review prior to the appointment—for more information, check out the resources at the bottom of this article. Here are the basic steps for patients:
Follow up injections
Evidence shows that patients’ self-injection skills improve with continuation and that patients who try self-injection prefer it to provider-injection. While patients are building skills, consider scheduling a telehealth visit for continued support on their injection dates. Patients can keep a log of their injection dates, so they know when the next injection is due, or they can set up reminders on their phone to stay on top of their next injection date.
DMPA-SQ can be taken anytime up to 14 weeks after the last DMPA-SQ injection, so it’s okay to give the next injection early. However, if it has been more than 14 weeks since the last DMPA-SQ injection and you can be reasonably certain that they are not pregnant, recommend self-injection of DMPA-SQ as soon as possible and using a backup method of birth control, such as condoms, for seven days.
Counseling tips
Safe storage
DMPA-SQ should be stored at room temperature (around 70 degrees), so it should not be put in the refrigerator, freezer, or left outside or in a car.
Disposing of needles
Used needles should be placed in a sharps’ container and cannot be thrown in the garbage. Patients can obtain a sharps’ container (usually for free) at most pharmacies by asking for one. If patients are unable to obtain a sharps’ container, you can prescribe one for them. Alternatively, patients can make a sharps’ container out of a strong plastic container that is labelled as a sharp container. Sharps’ containers can be disposed of at a drop off site.
Side effects
Proactive counselling about side effects has been shown to improve satisfaction and continuation. The most common side effect of DMPA is bleeding pattern changes, including unscheduled bleeding, and amenorrhea. Other side effects include weight gain, increased risk of diabetes in people with increased baseline diabetes risk, mood changes, headache, dizziness, bloating, and hair loss.
Let the patient know that they may have site irritation or pain with the first few injections, but it will likely improve over time. Users can consider applying ice to decrease sensation at the site before injecting. Additionally, the DMPA-SQ package insert notes that 1/100 people will experience dimpling at the site of injection.
DMPA carries a black box warning to not use for extended periods of time due to its effect on decreasing bone density; however, this decrease in bone density has not been associated with bone fractures, is not an indication for bone density testing, and bone mineral density loss is reversed after discontinuation of DMPA.
Paying for DMPA-SQ
Some private and public insurance companies do not cover DMPA-SQ and some require a prior authorization or approval. Patients can check with their insurance to see if it’s covered but you may need to contact the insurance company and advocate on behalf of your patient.
Bottom Line
DMPA-SQ is a great option for people who want to use the shot for birth control without going into a health care setting.
Additional Resources:
– Video for providers regarding prescribing and counseling about DMPA-SQ:
– National Family Planning & Reproductive Health Association (NFPRHA) DMPA-SQ Clinical Protocols and Resource Guide.
– RHAP Guidelines for DMPA-SQ self-injection, in multiple languages including English, Spanish, Vietnamese, Hindi, Simple and Traditional Chinese.
– UCLA/Harbour patient video about how to injection DMPA-SQ in English.
– RHEUMinfo patient video in English about DMPA-SQ injection.
– Written guidelines for patients in Spanish and English about DMPA-SQ self-injection from Planned Parenthood of Greater Texas.