



Estimated reading time: 6 minutes
A 28 year-old patient (she/her) calls the clinic asking for a refill. She’s had several “yeast infections” over the past year, sometimes it’s itchy, sometimes it just smells off. She’s tried over-the-counter antifungals, and you’ve prescribed an oral antifungal before, but nothing seems to stick. She’d rather skip the in-person visit if possible.
Sound familiar? Recurrent vaginitis is responsible for 6 to 10 million office visits per year and remains one of the more frustrating clinical problems to manage correctly. The Reproductive Health Hotline (ReproHH) team walks us through what providers need to know about diagnosis, treatment, and what’s changed recently.
Why can’t I diagnose and treat recurrent vaginitis over the phone?
It’s tempting, especially when a patient has a documented history of yeast infections and is requesting the same medication. But vaginitis is genuinely difficult to diagnose accurately without an in-person examination, and the stakes of getting it wrong are high.
One study recruited symptomatic patients at a pharmacy who were already purchasing antifungal creams. When offered same-day clinical exams, 50% were found to have a different infection entirely, and another 20% had mixed vaginitis — BV and candida together. That means 70% would have been treated inappropriately without in-person evaluation.
Skipping the exam also risks missing more serious diagnoses: desquamative inflammatory vaginitis (DIV), STIs, vulvar dermatoses, dysplasia or cancer, genitourinary syndrome of menopause or lactation, vulvodynia, or azole-resistant candida.
How do I tell bacterial vaginosis from a yeast infection?
The two most common causes of vaginitis–bacterial vaginosis (BV) and vulvovaginal candidiasis (yeast infection)–have distinct presentations, but they’re easy to conflate and can co-exist.
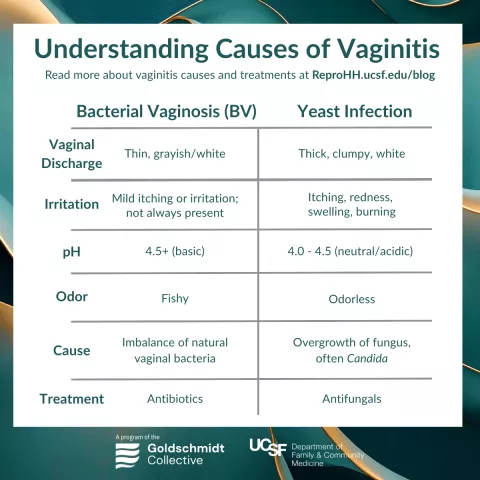
BV results from an imbalance of vaginal bacteria; yeast infections from an overgrowth of fungus, most often Candida albicans. Mixed vaginitis is common and easy to miss.
What are the diagnostic options for vaginitis?
Diagnosis can be made with point-of-care microscopy, molecular testing, and/or culture.
Point-of-care microscopy
- Same-day results.
- Particularly useful for diagnosing BV.
- Essential for a desquamative inflammatory vaginitis (DIV) diagnosis.
- Sensitivity and specificity are low for yeast infections.
- Not every clinic has a microscope or the capacity to use one in a busy clinical day.
Molecular testing (examples include BD Max, Aptima, NuSwab, and Xpert Xpress)
- More accurate and associated with lower follow-up costs.
- Access is still uneven, but worth advocating for in your clinical setting.
Yeast Culture
- Most useful for yeast speciation and sensitivities.
- Particularly helpful when azole resistance or non-albicans candida is suspected.
Self-Swab for Vaginitis
Self-collection is valuable for expanding access in resource-limited settings, reducing barriers related to pelvic examination, and enabling community-based screening. Traditional bedside diagnostic methods (Amsel criteria, wet mount) require clinician involvement, so the self-collection advantage is fully realized when specimens are processed using NAAT-based or Gram stain (Nugent scoring) methods rather than point-of-care clinical assessments.
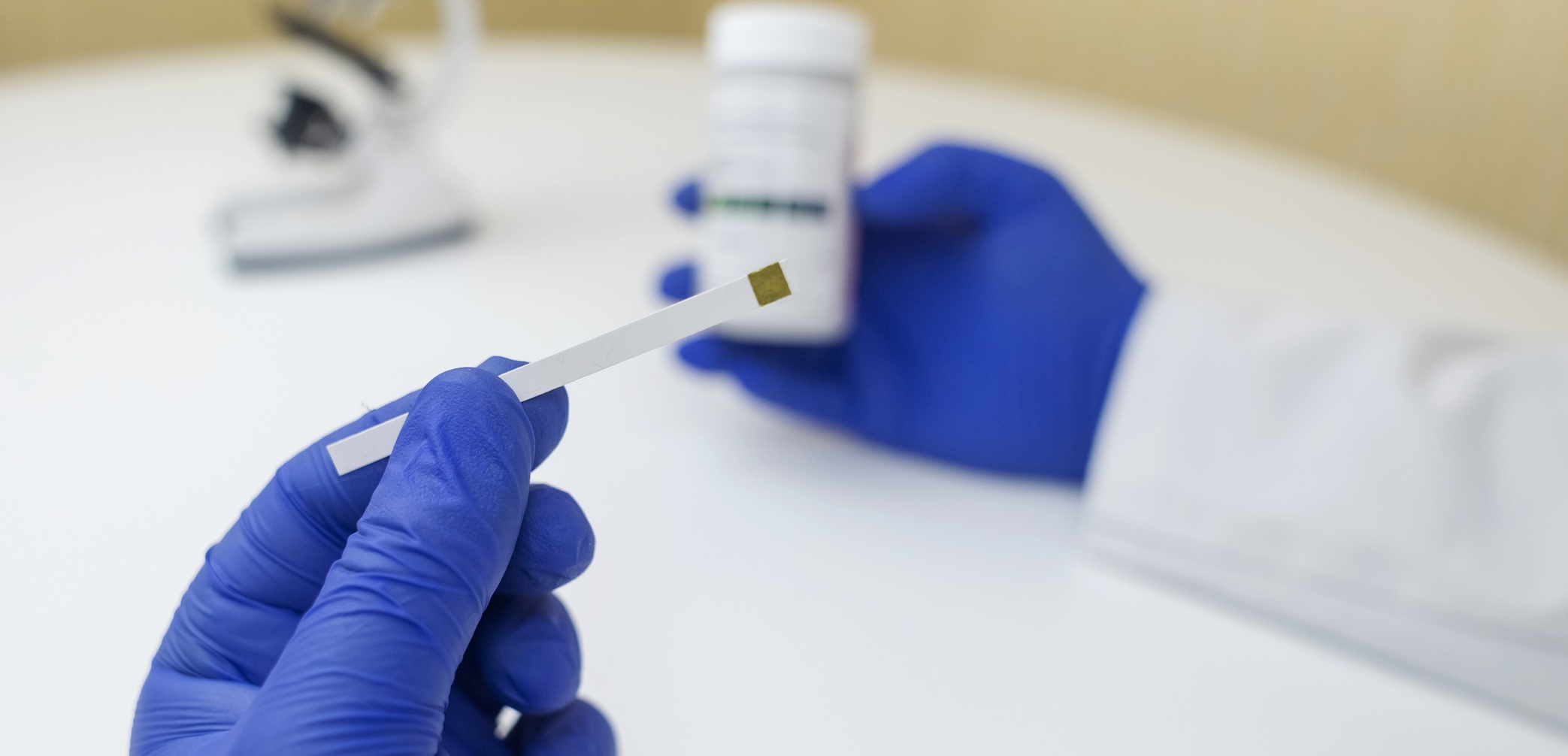
- Over-the-counter (OTC), at home testing method
- The only OTC method currently available is vaginal pH testing. The test uses a swab or paper strip that changes color when moistened with vaginal fluid, indicating vaginal pH.
- The test uses a swab or paper strip that changes color when moistened with vaginal fluid, indicating vaginal pH.
- Key limitation of this OTC test is that a pH >4.5 is suggestive of BV, while a normal pH helps rule it out. Elevated pH is not specific to BV — it can also be caused by trichomoniasis, atrophic vaginitis, semen exposure, or menstrual blood. A normal pH doesn’t exclude BV. Thus, this test can be used as a screening/triage tool and is not diagnostic.
- At-home NAAT kits
- Several at-home vaginal NAAT self-collection kits with mail-in laboratory processing are available.
- The tests include three FDA-cleared ones: BD Max Vaginal Panel, Aptima BV, and Xpert Xpress MVP; plus several laboratory-developed tests including NuSwab VG [LabCorp], OneSwab BV Panel [Medical Diagnostic Laboratories], and SureSwab BV [Quest Diagnostics]. These are validated for self-collected vaginal swabs in symptomatic patients and provide high-sensitivity, high-specificity molecular diagnosis of BV, candidiasis, and trichomoniasis.
How do I treat recurrent yeast infections?
Recurrent vulvovaginal candidiasis is defined as:
- three or more infections in one year,
OR - two or more in six months.
The standard induction regimen is fluconazole 150mg every 72 hours for three doses, followed by maintenance therapy: either a topical azole twice weekly or oral fluconazole weekly for six months.
Important caveats for managing recurrent vulvovaginal candidiasis long-term:
- More than 50% of patients may experience recurrence at one year, so some patients will need maintenance therapy beyond six months.
- Oteseconazole is a newer FDA-approved option, but it carries fetal toxicity risk. Patients must be using a highly effective contraceptive method during treatment and for an extended period after.
- For suspected azole-resistant or non-albicans candida, culture with sensitivities is essential before treatment. Vaginal boric acid (600 mg) for 21 days is often the most accessible alternative.
How do I treat recurrent bacterial vaginosis?
Recurrent BV is defined as:
- three or more episodes in one year.
Even with treatment, recurrence rates are high, with roughly 25% of patients experiencing symptom return by the end of treatment, and 50% recur within three months of completing a course.
First-line treatment for recurrent BV is weekly vaginal metronidazole for three months. Avoid prolonged oral metronidazole due to neuropathy risk.
Vaginal boric acid (600 mg daily for 14 days, followed by twice weekly for three months) is a strong alternative, particularly for patients with a history of mixed vaginitis.
Some patients benefit from a combination approach: oral metronidazole plus vaginal clindamycin or boric acid.
What’s new in recurrent BV treatment?
Data from the StepUp trial, published in the New England Journal of Medicine in early 2025, found that treating male partners with dual antibiotics (oral metronidazole plus topical penile clindamycin cream) reduced BV recurrence by more than half, from 63% to 35% over 12 weeks.
In response, ACOG issued a Clinical Practice Update in October 2025 recommending that clinicians consider concurrent sexual partner therapy for patients with recurrent, symptomatic BV who have male partners. The guidance also recommends shared decision-making about partner therapy for patients with same-sex partners and for those experiencing a first occurrence.
This is the first time ACOG has recommended partner treatment for BV, and it reflects a meaningful shift in how the field understands the role of sexual transmission in BV recurrence.
What about probiotics for BV prevention?
Patients often ask about this. Current evidence for most commercially available probiotics is weak for both BV and yeast infection prevention. However, research on a Lactobacillus crispatus-based vaginal suppository is promising. This strain dominates a healthy vaginal microbiome and a commercially available product is currently in development. For now, it’s reasonable to tell patients that most OTC vaginal probiotics aren’t well-evidenced for BV prevention, but that this is an area to watch.
When should I call ReproHH for help with recurrent vaginitis?
The ReproHH clinical consultation line is available for questions about recurrent vulvovaginal candidiasis, recurrent BV management, non-albicans yeast infections, partner therapy logistics, and newer antifungal options including oteseconazole.
Call 1-844-ReproHH (844-737-7644) after reviewing their Terms of Service.